


Cannabis is the cutting-edge drug for reform, the only politically plausible candidate for major legal change, at least decriminalisation (removal of criminal penalties for possession) and perhaps even outright legalisation (permitting production and sale). Compared with other drugs, the harms, physiological or behavioural, are less severe and the drug is better integrated into the culture. Throughout Western Europe and in the Antipodes there is pressure for reductions in the punitiveness of the marijuana regime.
This paper attempts to project the likely consequences of substantial changes in the basic legal regime for cannabis and to offer an assessment of those consequences. The best evidence on the effects of liberalising marijuana policy comes from The Netherlands which has experienced both decriminalisation and commercialisation, though without ever changing formal law. In this paper, we summarise and extend our analysis of the Dutch cannabis policy (Reference MacCoun and ReuterMacCoun & Reuter, 1997).
The Dutch experience, together with those of a few other countries with more modest policy changes, provides a moderately good empirical case that removal of criminal prohibitions on cannabis possession (decriminalisation) will not increase the prevalence of marijuana or any other illicit drug; the argument for decriminalisation is thus strong. Making cannabis fully legal is likely to increase its use substantially because of promotion, particularly in the USA with its peculiar dedication to commercial free speech; that is possibly undesirable. An intermediate model can be devised which may be preferable to either legalisation or simple decriminalisation.
DUTCH CANNABIS POLICY
In compliance with international treaty obligations, Dutch law states unequivocally that cannabis is illegal. Yet in 1976 the Dutch adopted a formal written policy of non-enforcement for violations involving possession or sale of up to 30 g of cannabis - a sizeable quantity, since few users consume more than 10 g a month (probably 25-35 joints) (Reference Cohen and SasCohen & Sas, 1998). In 1995, in response to domestic and international pressures, this threshold for possession was lowered to 5 g. Moreover, a formal written policy regulates the technically illicit sale of those small amounts in open commercial establishments; a 500 g limit on trade stocks was established in 1995. Enforcement against those supplying larger amounts is aggressive; in 1995 the Dutch government seized 332 tonnes of cannabis, about 44 per cent of the total for the European Union as a whole (Ministry of Foreign Affairs et al, 1995).
Between 1976 and 1986, a set of guidelines emerged stipulating that coffee-shop owners could avoid prosecution by complying with five rules: (a) no advertising; (b) no hard drug sales on the premises; (c) no sales to minors; (d) no sales transactions exceeding the quantity threshold; and (e) no public disturbances (Ministry of Foreign Affairs et al, 1995). In 1980, Ministry of Justice guidelines decentralised implementation, providing greater local discretion. As a result, enforcement became more lenient in Dutch cities, and somewhat stricter in smaller towns (Reference JansenJansen, 1991). The effect is illustrated graphically in Dutch geographer A. C. M. Jansen's (Reference Jansen1991) maps plotting cannabis coffee-shop locations in Amsterdam. He depicts nine locations in 1980, 71 in 1985 and 102 by 1988. (A location may correspond to more than one coffee shop.) Jansen notes that “the first coffee shops were usually situated in unattractive buildings in backstreets” (p. 69), but observes that over the course of the 1980s the shops spread to more prominent and accessible locations in the central city; they also began to promote the drug more openly.
The cumulative effect on these formal, quasi-formal and informal policies is to make cannabis readily available at minimal legal risk to interested Dutch adults. There are approximately 1200 coffee shops selling cannabis in The Netherlands (Reference Abraham, Cohen and van TilAbraham et al, 1999, p. 93). Most offer an international variety of marijuana and hash strains of varying potency levels. Gram prices are 5 to 25 guilders ($2.50 to $12.50) (Reference Kraan, Leuw and MarshallKraan, 1994) compared with US figures of $1.50 to $15.00. It is possible that the Dutch marijuana is of higher potency and ‘quality’, a much less well-defined term but one which experienced smokers use. No data are available in either dimension. The continued high price of marijuana in The Netherlands probably reflects the aggressive enforcement against large-scale growers and distributors.
OUTCOMES
In MacCoun & Reuter (Reference MacCoun and Reuter1997), we considered three key policy questions. Are levels of cannabis use higher in The Netherlands than in other Western nations? Did levels of cannabis use in The Netherlands increase following the 1976 depenalisation and subsequent de facto legalisation? And has the policy change weakened the statistical association between marijuana and use of other drugs? Here, we briefly summarise and extend those findings. In the final section, we clarify our interpretation of those findings and possible implications for US cannabis policy.
Prevalence of cannabis use in The Netherlands, USA, Denmark and Germany
At the very least, meaningful cross-sectional comparisons of drug use should be matched for survey year, measure of prevalence (lifetime use, past-year use, or past-month use), and age groups covered in the estimate. Failure to meet these criteria has led to grossly discordant comparisons in which, for example, rates among 12- to 17-year-olds in one country are compared with those among 18-year-olds in another, all being called adolescents or teenagers (e.g. Associated Press, 3 October 1997 (P. Recer; published under different titles in various US newspapers); Los Angeles Times, 26 July 1998 (R. Housman; letter)).
Our 1997 paper presented 15 comparisons that met these criteria. Table 1 extends the list to 28: 16 comparisons to the USA, three to Denmark, two to West Germany, one to Sweden, one to Helsinki, one to France, and four to the UK. We identified 15 comparisons in 1997. Here we add 13 additional comparisons. Some of these pre-date that paper but were unknown to us at the time it was written. Two others (lifetime use among those 12 and older in Tilburg and Utrecht in 1995) were omitted from that study by an oversight. Including the latter increases the amount by which the US rates exceed those in Utrecht (from a 0.3% difference to a 1.4% difference) and especially Tilburg (from a 3.4% difference to a 7.9% difference). This does not change our substantive conclusion that “US rates are… similar to that of Utrecht, and higher than that of Tilburg” (Reference MacCoun and ReuterMacCoun & Reuter, 1997, p. 49). All but two occur in the 1990s, during the period we have characterised as de facto legalisation, not just depenalisation. Four contrasts compare national estimates from The Netherlands and the USA; three show negligible differences between the two countries (within sampling error), while the newest estimate (Reference Abraham, Cohen and van TilAbraham et al, 1999) suggests that US prevalence is much higher. This discrepant result may be attributable to the inclusion of older adults in the latter comparison, or due to some difference between the Centre for Drug Research (CEDRO) (household) and Trimbos-institut (school-based) national survey methodologies. Twelve comparisons involve US national data and a Dutch city. Six contrasts pair the USA with an estimate from Amsterdam — a large urban setting with a visible drug culture. American surveys indicate little difference, on average, between large metropolitan samples and the USA as a whole (Substance Abuse and Mental Health Services Administration, 1979-1999), but the estimates in Table 1 suggest that Amsterdam has a higher fraction of marijuana users than smaller Dutch communities. US rates are basically identical to those in Amsterdam and Utrecht, and higher than those in Tilburg (Reference Langemeijer, Korf and RiperLangemeijer, 1997; also see Reference Abraham, Cohen and van TilAbraham et al, 1999).
Table 1 Comparing cannabis use in The Netherlands and other nations
| Age group | Year | Prevalence type | Dutch location | Dutch prevalence (%) | Contrast location | Contrast prevalence (%) | Difference (%) |
|---|---|---|---|---|---|---|---|
| Netherlands1 v. USA2 | |||||||
| 12 to 17 | 1992 | Lifetime | Netherlands | 12.6 | USA | 10.6 | 2.0 |
| Approx. 18 | 1992 | Lifetime | Netherlands | 34.5 | USA | 32.6 | 1.9 |
| Approx. 18 | 1996 | Lifetime | Netherlands | 44.0 | USA | 44.9 | -0.9 |
| 12 and older | 1997 | Lifetime | Netherlands | 15.6 | USA | 32.9 | -17.3 |
| Mean Dutch-US difference: | -3.6 | ||||||
| Tilburg3 (population 165 000) v. USA2 | |||||||
| 12 and older | 1995 | Past month | Tilburg | 2.4 | USA | 4.7 | -2.3 |
| 12 and older | 1995 | Past year | Tilburg | 4.0 | USA | 8.4 | -4.4 |
| 12 and older | 1995 | Lifetime | Tilburg | 13.9 | USA | 31.0 | -17.1 |
| Mean Tilburg-US difference: | -7.9 | ||||||
| Utrecht3 (population 235 000) v. USA2 | |||||||
| 12 and older | 1995 | Past month | Utrecht | 4.3 | USA | 4.7 | -0.4 |
| 12 and older | 1995 | Past year | Utrecht | 8.2 | USA | 8.4 | -0.2 |
| 12 and older | 1995 | Lifetime | Utrecht | 27.4 | USA | 31.0 | -3.6 |
| Mean Utrecht-US difference: | -1.4 | ||||||
| Amsterdam4 (population 700 000) v. USA2 | |||||||
| 12 and older | 1994 | Past month | Amsterdam | 6.7 | USA | 4.8 | 2.0 |
| 12 and older | 1994 | Past year | Amsterdam | 10.5 | USA | 8.9 | 1.7 |
| 12 and older | 1994 | Lifetime | Amsterdam | 29.1 | USA | 32.6 | -3.5 |
| 35 and older | 1994 | Past month | Amsterdam | 3.5 | USA | 2.3 | 1.2 |
| 35 and older | 1994 | Past year | Amsterdam | 5.8 | USA | 4.1 | 1.7 |
| 35 and older | 1994 | Lifetime | Amsterdam | 22.0 | USA | 25.4 | -3.4 |
| Mean Amsterdam-US difference: | -0.1 | ||||||
| Netherlands v. other European nations | |||||||
| Approx. 18 | 1990 | Lifetime | Netherlands5 | 28.0 | Copenhagen6 | 52.0 | -24.0 |
| 20 to 24 | 1994 | Past year | Amsterdam4 | 25.0 | Denmark7 | 16.0 | 9.0 |
| 25 to 29 | 1994 | Past year | Amsterdam4 | 18.2 | Denmark7 | 7.0 | 11.2 |
| 12 to 29 | 1990 | Lifetime | Amsterdam4 | 33.0 | W. Germany6 | 16.0 | 17.0 |
| 25 to 29 | 1994 | Past year | Amsterdam4 | 18.2 | W. Germany7 | 5.6 | 12.6 |
| 15 | 1996 | Lifetime | Netherlands8 | 29.0 | Sweden9 | 7.2 | 21.8 |
| 15 | 1992 | Lifetime | Netherlands8 | 18.1 | Helsinki6 | 10.0 | 8.1 |
| 16 to 59 | 1994 | Past year | Amsterdam4 | 13.7 | UK9 | 13.0 | 0.7 |
| 16 to 39 | 1994 | Past year | Amsterdam4 | 17.8 | UK9 | 8.0 | 9.8 |
| 15 to 16 | 1995-9 | Lifetime | Netherlands10 | 29.3 | UK11 | 41.0 | -11.8 |
| 15 to 16 | 1995-9 | Past month | Netherlands10 | 15.3 | UK11 | 24.0 | -8.8 |
| Approx. 18 | 1994 | Lifetime | Netherlands12 | 39.3 | France13 | 29.0 | 10.3 |
| Mean Dutch-European difference: | 4.7 | ||||||
| Mean after excluding Copenhagen comparison: | 7.3 | ||||||
| Mean after excluding Copenhagen and Sweden comparisons: | 5.8 | ||||||
Unfortunately, many of the available contrasts between The Netherlands and her European neighbours suffer from the same weakness, comparing rates for an entire nation as a whole to those in the largest city of another nation. On average, Dutch prevalence rates are about 5 percentage points higher than their European neighbours; a 7% difference if one excludes the extreme Copenhagen contrast; a 6% difference if one also excludes the extreme Sweden contrast. Additional evidence, presented below, suggests that in recent years The Netherlands has had higher rates than Oslo, Norway. On the other hand, much of this higher Dutch rate is attributable to comparisons limited to Amsterdam, and we have seen that Amsterdam has higher rates than Tilburg and Utrecht. On balance, we conclude that Dutch rates are somewhat lower than those of the USA but somewhat higher than those of some, but not all, of its neighbours. Amsterdam's level of marijuana use is comparable to that of the USA.
Trends in the prevalence of cannabis use
Did levels of cannabis use in The Netherlands increase following the 1976 depenalisation and subsequent de facto legalisation? We examined Dutch lifetime prevalence data from various sources between 1970 and 1996 (Reference MacCoun and ReuterMacCoun & Reuter, 1997). (Past-month or past-year prevalence estimates would be more informative but are scarce, especially prior to 1986.) The data for ages 16-17 and 18-20 come from a periodic national school survey (Reference de Zwart, Stam and Kuipersde Zwart et al, 1997); the data for ages 16-19 in Amsterdam come from a periodic city survey (Reference Sandwijk, Cohen and MusterdSandwijk et al, 1995); and the trend line for 1970-1983 reflects a synthesis of various early estimates based on a multivariate analysis by Driessen et al (Reference Driessen, Van Dam and Olsson1989).
The trend line implies that, among Dutch adolescents, cannabis use was actually declining somewhat in the years prior to the 1976 change and that the change had little if any effect on levels of use during the first 7 years of the new regime. Unfortunately, we lack data on the stringency of enforcement in the years immediately prior to the change in law, though the trend lines are fairly smooth and declining for at least 6 years prior to 1976.
In the 1984-1996 period, which we characterise as a progression from depenalisation to de facto legalisation, these surveys reveal that the lifetime prevalence of cannabis in Holland has increased consistently and sharply. For the age group 18-20, the increase is from 15% in 1984 to 44% in 1996; past-month prevalence for the same group rose from 8.5% to 18.5% (Reference de Zwart, Stam and Kuipersde Zwart et al, 1997). Is this an effect of the emergence of de facto legalisation?
Two comparison series offer insight: the US Monitoring the Future annual survey of high-school seniors (Reference Bachman, Johnston and O'MalleyBachman et al, 1998), and an annual survey of Oslo youth, aged 15 to 21 (Norwegian Ministry of Health and Social Affairs, 1997). The USA and Norway both strictly forbid cannabis sales and possession, and aggressively enforced that ban throughout the period. Note that because the Oslo survey has a broader age range, these estimates are more meaningful for comparing trends over time than absolute differences in prevalence in any given year.
The two comparison series behave very differently from the Dutch series, and from each other until 1992. The US rates increase until 1979 and then fall steadily and substantially until 1992, while the Oslo figures increase sharply only until 1972, and then fluctuate around a flat trend until 1992. Interestingly, during the period 1992 to 1996, all three nations have seen similar large increases, as have Canada (e.g. Reference Adlaf, Ivis and SmartAdlaf et al, 1995) and the UK (Table 1). This weakens the hypothesis that the Dutch increases from 1992 to 1996 are attributable to Dutch policies per se; the fact that comparable increases occurred in nations with such different legal risks highlights the important role of non-policy influences that are only poorly understood. Nevertheless, the increases in Dutch prevalence from 1984 to 1992 provide the strongest evidence that the Dutch regime might have increased cannabis use among the young. As is seen in Fig. 1, this was a period in which use levels were fairly flat in Oslo and declining in the USA. Available estimates also suggest flat or declining use during this period in Catalunya, Stockholm, Hamburg and Denmark (Reference HartnollHartnoll, 1994), Germany as a whole (Reference Reuband, Bühringer and PlattReuband, 1992), Canada (Reference Adlaf, Ivis and SmartAdlaf et al, 1995) and Australia (Reference MugfordMugford, 1992). Thus, unlike the widespread post-1992 rises, the 1984-1992 escalation seems (almost) uniquely Dutch. In only one other location was cannabis use clearly increasing during this period — Helsinki, where lifetime prevalence doubled among 15-year-olds between 1988 (5%) and 1992 (10%) (see Reference HartnollHartnoll, 1994).
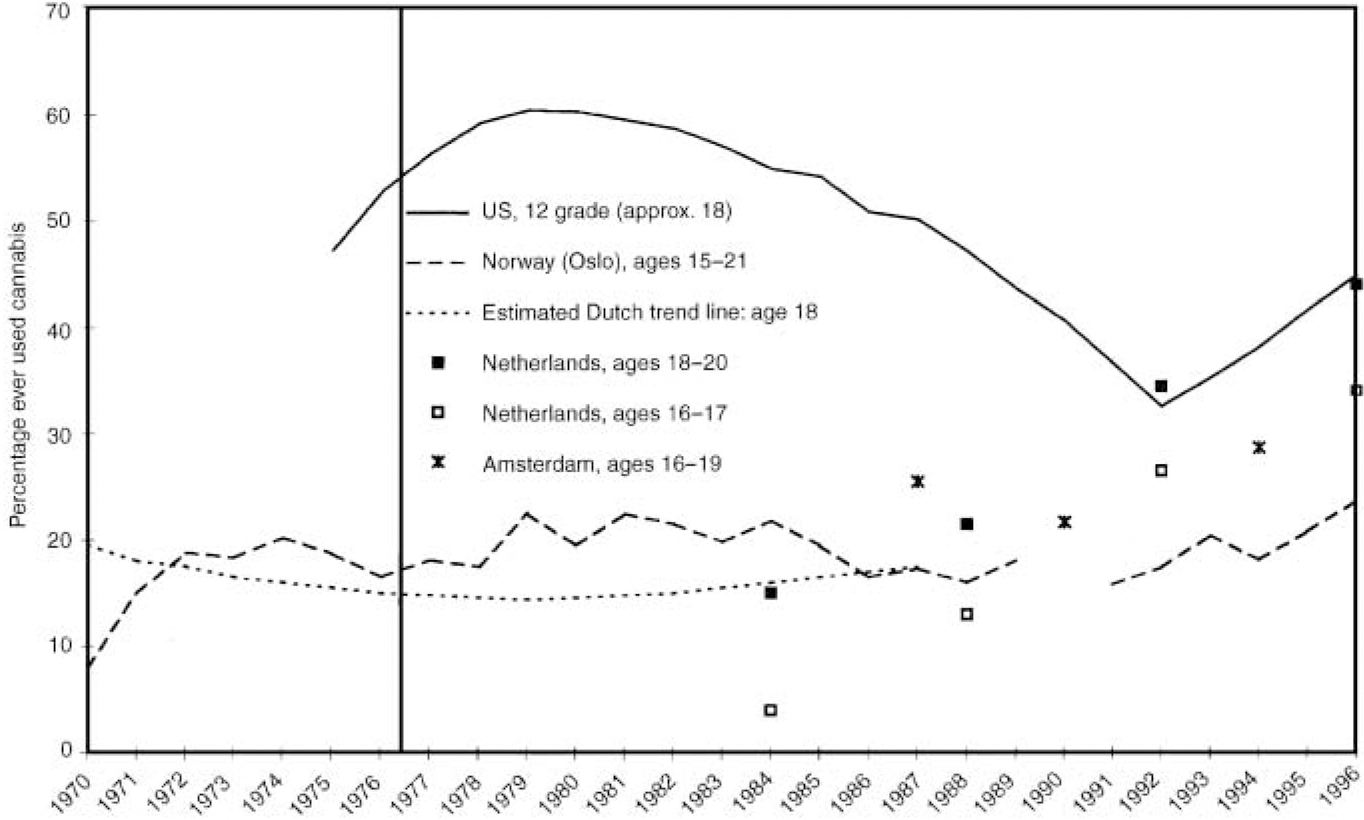
Fig. 1 Estimated lifetime prevalence of cannabis among 18-year-olds in the USA, The Netherlands, Amsterdam and Oslo.
Could the removal of criminal penalties for possession and small-scale sales require 8 years to have an effect? We hypothesise that the dramatic mid-1980s escalation in Dutch cannabis use is the consequence of the gradual progression from a passive depenalisation regime to the broader de facto legalisation which allowed for greater access and increasing levels of promotion, at least until 1995 when the policy was revised — in short, the effect of a shift from a depenalisation era to a commercialisation era.
We are not claiming that the increases circa 1984-1992 are solely attributable to coffee-shop commercialisation, nor that commercialisation is synonymous with coffee-shop transactions. Commercialisation also involves the heightened salience and glamorisation (in the youth-cultural sense) that results from widespread, highly visible promotion — the veiled references to cannabis in shop signs and advertisements, but also the explicit depictions in counter-cultural media ads, postcards and posters.
The gateway association
Has the Dutch policy change influenced the statistical association between marijuana and use of other drugs? Though American hawks argue that more lenient cannabis policies might lead to greater levels of hard-drug use, a central rationale for the 1976 Dutch legal change was the notion that separating the soft- and hard-drug markets might actually weaken any gateway effect (Ministry of Foreign Affairs et al, 1995). Dutch policy may have had some success in separating these markets. Most Dutch cannabis users obtain that drug through either coffee shops or friends; few buy from street dealers. According to the 216 experienced Amsterdam cannabis users interviewed by Cohen & Sas (Reference Cohen and Sas1998), hard-drug sales at coffee shops are quite rare; only four reported that cocaine could be purchased, and only one knew of heroin sales at a shop. Among past-year cannabis users aged 18 and older in The Netherlands as a whole, 48% cite coffee shops as their place of purchase; only 0.7% report purchases from strangers on the street (Reference Abraham, Cohen and van TilAbraham et al, 1999). Fewer than 2% of past-year cocaine users report buying cocaine at coffee shops.
In Amsterdam, as in the USA, almost all hard-drug users have used cannabis, but the vast majority of cannabis users have not used hard drugs. In both countries the surveys underestimate the number who frequently use cocaine or heroin and who almost certainly used marijuana. This reduces the denominator and numerator for calculating the percentage of marijuana users who went on to these other drugs; since the numerator is much smaller, this reduces the estimated rate below the true value. However, the problem holds in both nations and, since the Dutch are seen as doing a better job of integrating their addicts into the household population, may be less severe for The Netherlands than the USA. Only 22% of those aged 12 and over who have ever used cannabis have also used cocaine (Reference Cohen and SasCohen & Sas, 1996). This compares to a figure of 33% for the USA. For heroin, the corresponding figures are 4% for Amsterdam and 3% for the USA — statistically identical.
Thus, although the Dutch have failed to eliminate the statistical association between cannabis and hard-drug use — we estimate that the probability of cocaine or heroin use among those in Amsterdam who have never tried cannabis is essentially zero — it is possible that they have weakened it, at least for heroin. Also, only 6% of cannabis users had used cocaine more than 25 times; only 2% were current (past-month) users. Just 2% of cannabis users had used heroin more than 25 times; less than 1% were current users. Note, however, that the alleged gateway is a function of both the number of people who have tried marijuana and the probability of cocaine use given marijuana use. Any increase in the former component (the prevalence of marijuana use) might offset reductions in the latter component (the probability of moving on to cocaine use), and it is possible that Dutch commercialisation has had such an effect. From the perspective of breaking the gateway link, a regime that tolerates home cultivation of small quantities (as in Alaska and South Australia) might be more effective than the coffee-shop model.
The basis for continued cannabis prohibition
The case for continued prohibition of nonmedical uses of marijuana rests primarily on four possible harms: (a) marijuana's role as a gateway to other drugs of known dangerousness, a role generally believed to be unrelated to its legal status; (b) the health consequences and impact on adolescent development; (c) behaviour when intoxicated; and (d) the difficulty of quiting. We think none of these turns out to be very substantial; in particular, the gateway effect (which has seven possible interpretations) has probably been greatly overstated.
Our judgement, based on review of the research literature, is that at present the primary harms of marijuana use (including those borne by non-users) come from criminalisation: expensive and intrusive enforcement, inequity, shock to the conscience from disproportionate sentence and a substantial (though generally non-violent) black market. Certainly the drug itself causes damage: it generates accidents causing harm to both the user and others; regular use by adolescents may adversely affect development; it may have some substantial impact on the prevalence of cancer among frequent users; a non-trivial share of users has difficulty quitting when they wish to and see their lives as somewhat harmed because of their dependence. But the adverse consequences of criminalisation, at least with current US enforcement, seem more substantial.
The available evidence suggests that removal of the prohibition against possession itself (decriminalisation) does not increase cannabis use. In addition to the Dutch experience from 1976 to 1983, we have similar findings from analysis of weaker decriminalisations (with fines retained for the offence of simple possession of small quantities) in 12 US states (Reference SingleSingle, 1989) and South Australia and the Australian Capital Territory (Reference HallHall, 1997; Reference McGeorge and AitkenMcGeorge & Aitken, 1997). The fact that Italy and Spain, which have decriminalised possession for all psychoactive drugs, have marijuana use rates comparable to those of neighbouring countries provides further support. This prohibition inflicts harms directly and is costly. Unless it can be shown that the removal of criminal penalties will increase use of other more harmful drugs, perhaps because of the signal of lessened disapproval, it is difficult to see what society gains.
Decriminalisation is normatively flawed (why does sale remain illegal?) and still leaves the harms of black markets. However, the removal of the sales prohibition has more complex effects. We believe that it would generate larger increases in marijuana use as a result of promotion by the legal suppliers. Promotion could not be effectively limited in the US commercial marketplace for a product which, with no therapeutic goal, would be provided in conventional commerce rather than through doctors and pharmacies. Recent experience with legalised gambling, as well as the difficulty of suppressing cigarette promotion, added to the post-World War II erosion of repeal's liquor controls, all suggest that legal commercial interests are likely to weaken regulatory efforts. This is especially plausible for marijuana, whose harms are relatively slight, hence complicating the task of defending stringent regulation against the efforts of a legal industry. If, even with relatively tight regulation, The Netherlands saw a large increase in marijuana prevalence, US legalisation might lead to very high prevalence rates indeed. The increase in marijuana use would have to be weighed against the reduced intrusiveness of the state, reduction of black markets and possible substitution of marijuana for alcohol, which might be net health enhancing.
Other regimes between decriminalisation and commercialisation are possible. For example, the state of Alaska permits home production for own consumption and gifts to others. The impact on prevalence is difficult to determine (Reference SegalSegal, 1990) but it may be an appropriate compromise between the excess of commercialisation and the barren rights of decriminalisation. Our purpose here is not to choose an optimal regime but only to suggest that available evidence provides a basis for a reasonable debate about the likely consequences of regime changes.
Clinical Implications and Limitations
CLINICAL IMPLICATIONS
-
▪ It is important to distinguish depenalisation from commercialisation when assessing alternative to drug prohibition.
-
▪ The elimination or steep reduction in penalties for cannabis possession does not appear to influence cannabis prevalence.
-
▪ Legal or quasi-legal commercial sales of cannabis may produce significant increases in cannabis prevalence.
LIMITATIONS
-
▪ Cross-national surveys differ with respect to language, question wording, sampling, and other details that may bias inferences about relative cannabis prevalence.
-
▪ Cross-national differences in cannabis prevalence do not necessarily reflect national differences in cannabis policies.
-
▪ Existing sources of data on national cannabis use permit only weak forms of causal inference; observed correlations might be spurious.



eLetters
No eLetters have been published for this article.