


Disasters are neither new nor rare, yet it is only in the past two decades that post-traumatic reactions have been investigated systematically (Reference AlexanderAlexander, 1996). Major catastrophes represent important opportunities to examine the responses of individuals to a single, extreme, well-defined stressor. This allows investigation of variables within the disaster unique to each individual's experience. In particular, major catastrophes afford the opportunity to study the interaction between features of the traumatic event, the individuals and their circumstances in relation to outcome (Alexander, Reference Alexander1991, Reference Alexander, Wilson and Raphael1993). We performed a unique long-term follow-up of the survivors of the world's worst oil platform disaster to assess the long-term effects of major trauma. The role of factors relating to trauma, the survivors and the survivors' circumstances in the occurrence of general and specific post-traumatic psychopathology were investigated.
The Piper Alpha oil platform disaster took place on 6 July 1988, resulting in the deaths of 167 men and leaving 59 survivors. It involved the complete destruction above sea level of the platform at 193 km northeast of Aberdeen, a city in the Grampian region of Scotland. The crew were exposed to a range of extreme stressors, for example: toxic fumes, fire, being trapped, extended threat to life either on the platform or in the sea, witness to the injury to and/or the death of others, traumatic bereavement, and delayed rescue and medical care. Further details are available elsewhere (Alexander, Reference Alexander1991, Reference Alexander, Wilson and Raphael1993).
METHOD
Subjects
Of the survivors 78% (46/59) could be traced and were invited by letter in August, 1998, to take part in the study. No previous follow-up of the survivors had been conducted, to ensure that the senior investigator (D.A.A.) had concluded all clinical responsibilities to the survivors and to allow sufficient time for all compensation and legal proceedings to be completed. Therefore the long-term follow-up involved an uncontaminated sample from a research perspective. We avoided contacting individuals close to the ‘anniversary’ of the disaster. The study was approved by the Grampian Research Ethics Committee.
Disaster research has in the past compared survivors with a control group who have not experienced the traumatic event. This will only produce information about specific aspects of the event if the experimental and control groups vary in just one dimension (Reference Holen, Wilson and RaphaelHolen, 1993). It was not possible to generate such a control group for this study.
Assessments
Semi-structured interview
This was divided into sections and collected information on a number of areas, including: sociodemographics; concurrent stresses; detailed and specific questions about aspects of the subjects' personal experience of the disaster; physical problems and their care; post-traumatic psychosocial problems and their management; and employment problems. Physical injuries were further investigated by case-note review.
Self-report outcome measures
The Impact of Event Scale — Revised (IES—R; Reference Marmer, Weiss, Wilson and KeaneMarmer & Weiss, 1997) is a widely used, valid and reliable 22-item scale measuring subjective distress caused by intrusion (e.g. flashbacks and nightmares), avoidance and hyperarousal. It provides a total score (range 0-88).
The Post-Traumatic Symptom Scale (PTSS—12; Reference Holen, Wilson and RaphaelHolen, 1993) is a 12-item scale validated on a similar post-disaster population (the survivors of the Alexander L. Keilland oil platform disaster), and is designed to measure certain post-traumatic phenomena (e.g. irritability and impaired concentration).
The General Health Questionnaire — 28 (GHQ—28; Reference Goldberg and HillierGoldberg & Hillier, 1979) is a 28-item research version of the GHQ that provides a measure of general psychopathology. Using the conventional binary GHQ scoring method (range 0-28), we defined a total GHQ score ≥4 as indicative of ‘psychiatric caseness’ (i.e. if a clinical interview were undertaken a psychiatric diagnosis would be highly likely). For some analyses the total score was used as a continuous variable.
The Hopelessness Scale (Reference Beck, Weissman and LesterBeck et al, 1974) is a 20-item, well-established scale that provides a subjective measure of hopelessness with a total score (range 0-20).
Diagnostic interview
The Clinician Administered Post-Traumatic Stress Disorder (PTSD) Scale for DSM—IV, Current and Lifetime Diagnostic Version (CAPS—DX; Reference Blake, Weathers and NagyBlake et al, 1995) is a highly structured interview. It measures the frequency and intensity of the 17 DSM—IV (American Psychiatric Association, 1994) symptoms of PTSD (each scored 0-4), five associated features (each scored 0-4), social and work impact, global improvement, and severity (each scored 0-4). Both acute and current symptoms were assessed. For the purposes of this study we used the most stringent empirically derived scoring rule (Reference Weathers, Ruscio and KeaneWeathers et al, 1999) to convert the continuous severity scores into dichotomous categories for the analyses of the data. This rule, F1/12/SEV65 (i.e. a significant level of PTSD symptom severity and a distribution of symptoms corresponding to DSM—IV diagnostic criteria), was chosen to confirm an unequivocal diagnosis of PTSD in view of the relatively small number of survivors, to avoid false positives. This PTSD diagnosis and the total CAPS-DX scores were used in the analyses.
Procedure
Subjects were interviewed by a clinician experienced in the diagnosis and assessment of PTSD (A.M.H.), using the specially designed semi-structured interview and the CAPS—DX. The four self-report questionnaires were also administered at the time of the interview.
Statistical analysis
SPSS for Windows, version 9 (SPSS Inc, Chicago, IL) software was used to input and to analyse the data. Non-parametric methods were needed owing to skewed distributions and heterogeneity of variance. The Mann—Whitney U-test (corrected for ties) assisted between-group comparisons. Differences for paired data were analysed by means of the Wilcoxon matched pairs signed rank test. The relationship between variables was assessed by means of Spearman's rank correlation coefficient, the McNemar test for matched samples, and the χ-squared test for association, including Fisher's exact test when expected values were less than 5. All probability values relating to the hypotheses were one-tailed. Because of the risks of multiple comparisons generating spurious findings, only those with a probability value of 1% or less were considered significant. The results of all other data analyses are available upon request from the authors.
RESULTS
Subjects
Of the 46 subjects, 78% (36) agreed to contribute to the study, either by postal questionnaire (3 individuals) or by meeting with one of the investigators (A.M.H.) (33/36), as shown in Fig. 1. The interviews took place between August 1998 and December 1999. There were no significant differences between participants and non-participants for age and home location (Table 1). The duration of time worked offshore either on Piper Alpha or on other installations was not available for non-participants.
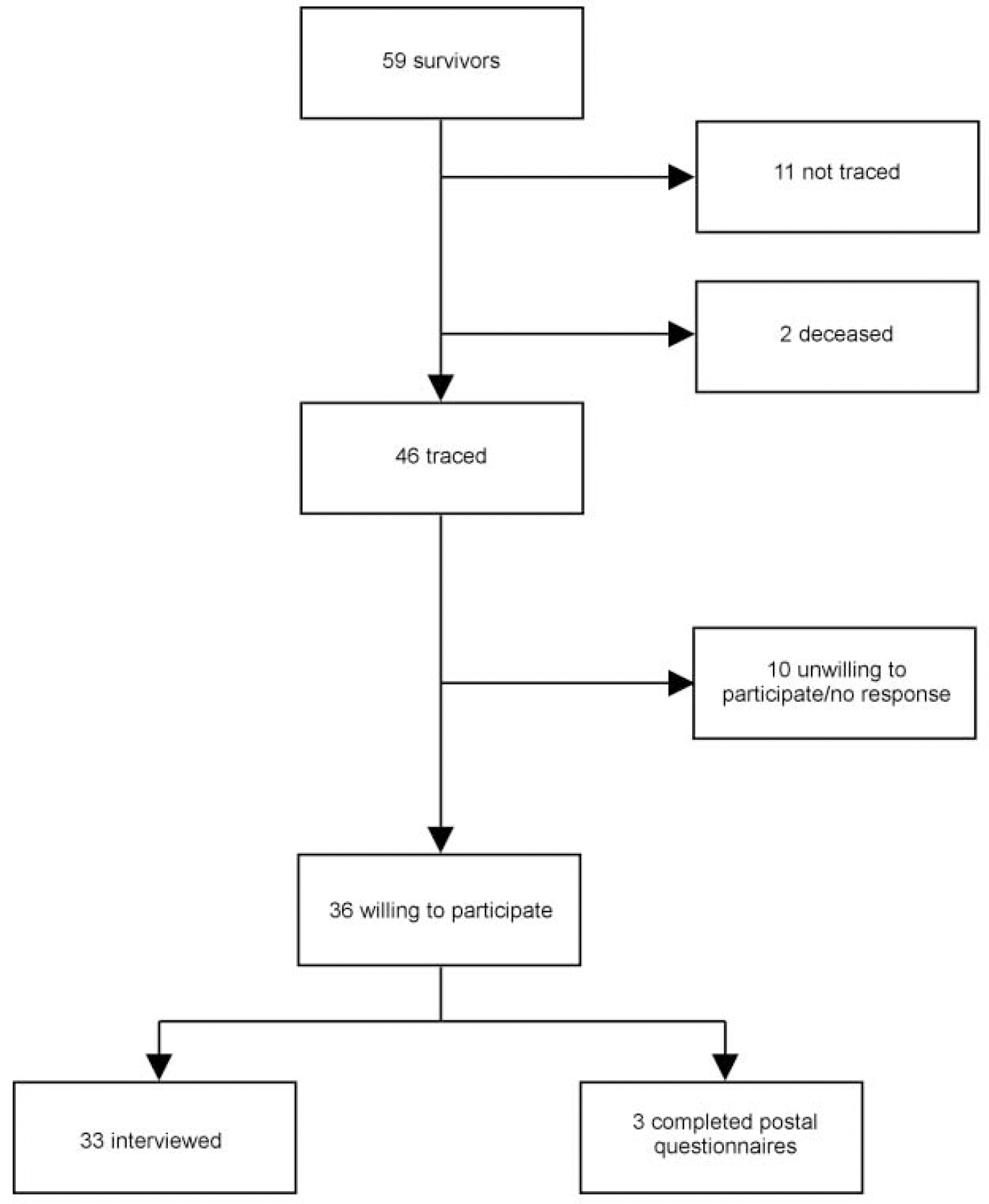
Fig. 1 Study profile.
Table 1 Demographic characteristics of the participants and non-participants
| Characteristic | Participants (n=36) | Non-participants (n=23) |
|---|---|---|
| Age (years) | ||
| Median | 36.5 | 37.0 |
| Range | 22-58 | 23-56 |
| Home location (time of disaster) | ||
| Grampian | 10 | 11 |
| Scotland (excluding Grampian) | 14 | 3 |
| Other (outside Scotland) | 12 | 9 |
| Time offshore (years) | ||
| Median | 9.75 | - |
| Range | 3-20 | - |
| Time on Piper Alpha (years) | ||
| Median | 2.25 | - |
| Range | 0-15 | - |
Prevalence of PTSD and other psychological symptoms
As measured using the scoring rule F1/12/SEV65, 21% (7/33) had a current diagnosis of PTSD and 73% (24/33) had a diagnosis of PTSD using this same rule for symptoms reported in the first 3 months after the disaster. In addition, survivors with sustained anger, as measured on the CAPS—DX, had significantly higher current post-traumatic symptoms on the PTSS-12 scale (z=-2.949; P=0.01) and diagnostic interview (z=-2.636; P=0.01). Survivors had median IES—R and PTSS—12 scores of 19 (range 0-60) and 6 (range 0-12), respectively.
Current GHQ—28 ‘caseness’ was 44% (16/36). As measured by the semi-structured interview, 76% (25/33) of the survivors stated that they had experienced psychological problems within 1 month, with symptoms starting within 3 months in 97% (32/33). In addition, 64% (23/36) stated that some of their psychological problems were still present. Survivors had a median Hopelessness Scale score of 4, with a range of 0-15.
More than one-third (36%; 12/33) of survivors described survivor guilt (‘I should not have survived’) after 10 years, and 70% (23/33) reported acute guilt. Survivors who experienced acute survivor guilt were significantly more likely to have severe acute PTSD, as measured by CAPS—DX (Fisher's exact test, P=0.001). Similar findings were evident for performance guilt (‘I should have done better’); 33% (11/33) had performance guilt currently and 61% (20/33) had the symptom acutely. Survivors with acute performance guilt were significantly more likely to have severe acute PTSD (Fisher's exact test, P=0.01), and those with sustained performance guilt had significantly higher rates of PTSD on the CAPS—DX (Fisher's exact test, P=0.01). McNemar tests on survivor and performance guilt each had a significance level of P=0.01, indicating that symptom severity and occurrence decreased over time. Survivors who reported chronic dissociative symptoms were significantly more likely to have post-traumatic symptoms on the PTSS-12 (z= -2.77, P=0.01) and on the CAPS—DX (Fisher's exact test, P=0.01), and to have higher Hopelessness Scale scores (z= -2.9, P=0.01).
Personal experience
The majority of survivors (97%; 35/36) experienced the loss of a friend; 86% (31/36) thought they might die; 86% (31/36) saw someone who had been seriously injured or killed; and 58% (21/36) saw someone being killed or injured. Survivors who saw the death of and/or injury to colleagues had significantly higher IES—R scores (z= -2.47, P=0.01) and higher total CAPS—DX scores (z= -2.88, P=0.01). There were no significant associations between delayed rescue and general or specific post-traumatic symptomatology.
Physical injury
The majority of participants were physically injured (83%; 30/36), with 56% (20/36) sustaining more than one injury and 42% (15/36) requiring hospital admission. Survivors who jumped from the platform were significantly more likely to have burns (χ2=7.67, d.f.=1, P=0.01), as were those who spent longer periods in the water (χ2=6.52, d.f.=1, P=0.01). Survivors who sustained fractures during the disaster had significantly higher post-traumatic symptom scores on the IES—R scale (z= -2.781, P=0.01). No other statistically significant association was found between the nature and/or extent of physical injury and the prevalence or severity of PTSD.
Social and occupational functioning
The majority of survivors (78%; 28/36) reported difficulties finding work post-trauma; these survivors were significantly more likely to report higher post-traumatic symptom scores on the IES—R (z= -3.065; P=0.001) and had significantly more severe acute PTSD symptoms at diagnostic interview (χ2=8.80, d.f.=1, P=0.01). Survivors meeting diagnostic criteria for PTSD, both acutely and currently (as measured by CAPS—DX), had significantly greater impairment in social and occupational functioning (z= -3.61, P=0.001).
Stressors
The prevalence of pre-trauma stressors was generally low, the most common being marital disharmony (42%, 14/33), employment difficulties (27%, 9/33) and bereavement (27%, 9/33). Participants with accommodation problems before the disaster were significantly more likely to meet GHQ-28 caseness (Fisher's exact test, P=0.01). Survivors with a pre-trauma history of physical illness in a family member had significantly higher IES—R scores (z= -2.539; P=0.01), but no other stressor was significantly related to any outcome measure either singly or combined. McNemar tests on all areas of concurrent life stresses indicated that for each variable the extent of the problem increased after the disaster (P=0.01). The effects of traumatic events that occurred either before or after the disaster could not be tested statistically as only 2 subjects had experienced another traumatic event. Survivors meeting GHQ caseness currently (10 years post-trauma) were significantly more likely to have developed alcohol problems (Fisher's exact test, P=0.01) or financial problems (Fisher's exact test, P=0.01) after the disaster.
Treatment and support systems
Psychological problems were reported by 97% (32/33) of survivors, with 76% (25/33) subsequently having individual therapy; 55% (18/33) prescribed medication; 21% (7/33) group psychotherapy; and 55% (18/33) a combination of treatments (Table 2). Having treatment was associated with having a diagnosis of acute PTSD (Fisher's exact test, P=0.01). The ease of access to treatment varied considerably for group psychotherapy, but both individual therapy and medication were readily available to the majority of those who used them. A support group in Aberdeen and the helpline were both viewed as helpful by the large majority of participants who used them (Table 2). A reunion held 12 months after the disaster was viewed as helpful by most who attended it (Table 2).
Table 2 Perceived helpfulness of the treatment and support system used
| Helpful | ||
|---|---|---|
| % | n | |
| Treatment | ||
| Individual psychotherapy | 44 | 11/25 |
| Group psychotherapy | 14 | 1/7 |
| Medication | 28 | 5/18 |
| Support services | ||
| The helpline | 93 | 13/14 |
| The support group | 83 | 15/18 |
| The reunion | 83 | 20/24 |
Worst long-term effects
The majority of survivors (61%, 22/36) stated that the worst long-term effect of the disaster was its impact on their emotional and psychological well-being and on their relationships. Only 8% (3/36) stated that situational problems (e.g. financial difficulties) were the worst long-term effects of the disaster.
Positive aspects
Of survivors interviewed, 61% (22/36) stated that some good had come of the experience, with 44% (16/36) identifying changes in emotional and personal life (e.g. closer to family, more emotionally expressive), and 17% (6/36) specifying situational changes (e.g. financial security through compensation) as the main positive effects.
DISCUSSION
Prevalence of PTSD and other psychological symptoms
This 10-year follow-up of the Piper Alpha oil platform disaster highlights the long-term impact of a major disaster on the psychosocial functioning of individuals. The rates of psychological morbidity in this study are consistent with general levels of psychological morbidity after other mari-time disasters (Reference RaphaelRaphael, 1986) but are much higher than in Holen's study of the survivors of the Alexander L. Keilland oil platform disaster (Reference Holen, Wilson and RaphaelHolen, 1993). However, the two groups of survivors from these oil platform disasters had very different trauma experiences; for example, rates of physical injury were much higher in our study. It is interesting to note that, although we found no difference between subjects with persistent physical consequences and those with acute injuries which had not led to lasting physical disability, others such as Ehlers et al (Reference Ehlers, Mayou and Bryant1998) have found persistent physical consequences to be of considerable prognostic significance. Furthermore, the current level of GHQ caseness was 44%, which compares with reports of GHQ caseness in the general population of 18% (Reference Hardy, Shapiro and BorillHardy et al, 1997). The majority of survivors in this study had improved symptomatically but many still had a persistent diagnosis of PTSD or had some post-traumatic symptoms that no longer met the most stringent criteria for the diagnosis.
A major issue in trauma research is the validity of symptom reporting and the accuracy of recall of traumatic events. Are the survivors the best source of accurate information about the stressor? Their psychological adjustment may colour their recall of events, and the accuracy of recall of traumatic events has been found to decay over time (Reference McFarlaneMcFarlane, 1988). However, corroboration was available for a large proportion of the accounts of the individual survivors' personal experience from other survivors, with reassuring consistency. Furthermore, data about the Piper Alpha disaster were collected soon after the event in both clinical settings and the legal inquiry. In trauma research, particularly in long-term follow-up studies, this is unusual.
Traumatic events also affect social and occupational functioning adversely. The high levels of post-traumatic reactions found in this group only partially relate to features of the stressor itself, such as physical injury and witnessing injury or death, or its aftermath. A complex interrelationship exists between features of the trauma, the characteristics of the survivor (e.g. sustained guilt or anger) and the survivor's circumstances (e.g. lack of support or perceived lack of control).
Guilt would appear to be one of the central and most chronic symptoms of PTSD. Green (Reference Green, Davidson and Foa1993a ) has stated that guilt is infrequent and, if ranked, would have tied for last place among the PTSD symptoms of survivors after the Buffalo Creek flood. In our study, performance and survivor guilt were found to be not only persistent and severe symptoms but strongly associated with severe acute PTSD and enduring PTSD. Van der Kolk (Reference van der Kolk1996) and others have suggested that exposure therapy (facing the feared situation or traumatic memory either in vivo or in fantasy) in the presence of guilt may worsen both shame and guilt. This may explain the adverse effects of exposure found by Pitman et al (Reference Pitman, Altman and Greenwald1991). The presence of guilt must be identified before the use of exposure therapy, to prevent the exposure itself having a psychonoxious effect. Early guilt will both encourage, and be further exacerbated by, a negative appraisal of the traumatic event. The identification and treatment of guilt would appear to be important in facilitating the survivor's ability to recover. Furthermore, the importance of the recognition of guilt is highlighted by research demonstrating that guilt is the most significant explanatory factor in suicidal behaviour in combat veterans with PTSD (Reference Hendin and HaasHendin & Haas, 1991). Non-trauma specialists may not enquire about guilt as it is not classified as one of the central symptoms of PTSD; concentrating solely on the core criteria for the diagnosis of PTSD will give a restricted view of the impact of the trauma and of the necessary management for the victim of the traumatic event. Guilt and dissociative symptoms are currently termed associated symptoms of PTSD rather than core criteria, but our study would suggest that both are strongly associated with the development of both acute and chronic PTSD.
Personal experience
Threat to life has been shown to be a significant predictor of long-term outcome (Reference Green, Wilson and RaphaelGreen, 1993b ) but threat to life was so prevalent in our study (86%) that analysis was not possible. Exposure to the grotesque, such as seeing the death of, or injury to, another person, has been shown elsewhere to be highly disturbing (Reference Green, Wilson and RaphaelGreen, 1993b ). Traumatic bereavement, particularly if the person is present at the time of the death, is predictive of PTSD across a wide variety of events (Reference Green, Wilson and RaphaelGreen, 1993b ). The vast majority (97%) of Piper Alpha survivors experienced such loss, often of large numbers of close workmates and friends. Physical injury is seldom examined in research on traumatic events despite its relationship to threat to life. Our study shows the association of physical injury with PTSD and hopelessness, and thus emphasises the need for close liaison between surgeons and physicians, and their mental health colleagues.
The traumatic event was not universally and equally stressful for all survivors. Researchers must examine the specific aspects of such individual's experience rather than overgeneralising about the effects of traumatic events (Reference Holen, Wilson and RaphaelHolen, 1993). Any disaster may have unusual characteristics, and the evaluation of the characteristics of the stressor is essential to allow the application of the findings to other trauma populations.
Social and occupational functioning
Re-employment difficulties for survivors were significantly associated with poorer outcome. Survivors acknowledged many diverse reasons for employment problems beyond their psychological and physical injuries, such as experiencing prejudice in the workplace as a result of being a survivor of the Piper Alpha disaster. The ability to adjust to working offshore again was related to better outcome: a large proportion of the survivors (33%; 12/36) had worked offshore again despite the extent of the disaster and the rates of physical injury. For some this was only for a brief period, but others returned to offshore work within weeks and continued in similar jobs. This might have been the result of a lack of other marketable skills, of the need as reported by survivors to get ‘back on the horse’ or a re-enactment of the trauma (Reference van der KolkVan der Kolk, 1989). Survivors reported a restriction of social interaction and lessening of interest in their previous leisure pursuits after the disaster, which persisted for many survivors for more than 10 years.
Treatment and support systems
A coordinated and flexible response to major disasters is critical. It was reassuring to find that survivors of Piper Alpha were both aware of the need for treatment and were able to access it where they lived. Over 81% (29/36) received at least one form of treatment and many (69%; 25/36) also made use of the support system (e.g. the support group and the helpline) and other non-professional help (82%; 27/33). The helpline and the support group were found to be helpful by the large majority of survivors who used them. The one complaint regarding the support group was its distance from some of the survivors who lived geographically far from Aberdeen, some outside Britain. Some of the survivors living further from the centre of interest and support reported feeling isolated, although some had actively sought isolation from other survivors and from the media coverage.
The men had a varied experience of professional treatment, with approximately three-quarters (76%) having individual therapy and over half having a combination of treatments. Survivors who made use of treatment for psychological symptoms were those who reported severe acute post-traumatic symptoms. The survivors' symptoms and level of functioning had improved over the 10-year period, with fewer individuals having specific symptoms such as survivor and performance guilt and fewer meeting PTSD diagnostic criteria. These findings are similar to research by others such as Kessler et al (Reference Kessler, Sonnega and Bromet1995), who found a shorter duration of symptoms (3 years) among those who obtained professional help than among those who did not (5 years).
Strengths and limitations of the study
A strength of our study is that we examined an unselected survivor population; all survivors were invited to participate. The participation rate was high, with 78% of survivors who could be traced agreeing to take part. Research elsewhere, most notably by Weisæth (Reference Weisæth1989), has shown that resistance to initial interview and examination was related to severity of exposure and to the presence of post-traumatic stress reactions. Weisæth has argued that the true prevalence of PTSD would be underestimated unless response rates were high. The number of subjects in this study is small as a result of the small number of survivors of the disaster; also, the survivors may represent a sub-group of individuals who behaved in ways likely to optimise their survival (Reference WeisæthWeisæth, 1984).
Trauma research is bedevilled by ethical and methodological constraints imposed upon researchers. Any approach needs careful planning, yet rarely is there sufficient time to devise elegant research strategies. In pursuit of information there is the perennial risk of re-traumatising survivors by exposing them to distressing recollections of their trauma at interview. To limit the potential for our contact to cause distress we were careful to avoid the anniversary of the disaster because, as highlighted by Ehlers & Clark (Reference Ehlers and Clark2000), symptom-reporting rises at such a time. In addition, we gave participants the option of completing postal measures if they believed an interview might prove too distressing. Three survivors chose to participate in the study by this means. Some of the interviewed survivors did report an increase in intrusive symptoms both at the time of the interview and in the week preceding it. An assessment of the validity of responses is included in the CAPS-DX and was found to be high for the participants in this study. There was also a high rate of consistency between self-report measures and diagnostic interview. We are aware that the assessment of lifetime PTSD at the same time as the report of current symptoms may have led to a retrospective bias in symptom reporting.
There are several aspects relating to the data collected and reported that should be considered. The personal characteristics of the crew of the Piper Alpha are important in understanding their post-trauma reactions. The crew of the Piper Alpha platform were all male, a self-selected group (unlike transportation disaster victims), accustomed to both the onshore/offshore pattern of work and to spending long periods of time with close workmates. The crew can be considered to have been screened for some of the vulnerability factors for psychological illness, such as preexisting physical illness, which may account for the low levels of concurrent stressors the survivors reported at the time of the disaster. The work pattern might also have encouraged the development of other vulnerability factors such as alcohol misuse (Reference Ruch and LeonRuch & Leon, 1983) but this was not evident from self-reports in this study; only three men stated that they had had alcohol problems before the disaster. We acknowledge that the absence of corroboration of the subjects' alcohol intake might have led to an underestimation of the prevalence of alcohol problems.
Although survivors of the Piper Alpha disaster experienced high levels of general and specific post-trauma psychosocial morbidity, the majority (61%; 20/33) identified something positive to have come from the tragedy, whether personal or situational. This would not be consistent with the cognitive model proposed by Ehlers & Clark (Reference Ehlers and Clark2000), which proposes that individuals with persistent PTSD are unable to see the trauma as a time-limited event that does not have global implications for their future. Clearly this is an issue to be clarified by further empirical research. In general the participants were of the opinion that lessons learned from large-scale disasters resulted in improved response to traumatic events and treatment techniques for survivors; it is to be hoped that this is in fact the case. Professionals must also be alert to factors that might be modified to improve the short-term and long-term outcome for survivors of traumatic events.
CLINICAL IMPLICATIONS
-
▪ Assessment of the impact of a disaster must include more than the assessment of the core criteria for post-traumatic stress disorder (PTSD). Guilt, dissociative symptoms and re-employment difficulties were strongly associated with post-traumatic psychological difficulties.
-
▪ The majority of survivors will improve symptomatically over 10 years but many will have persistent post-traumatic symptoms.
-
▪ Despite high levels of psychological symptoms a majority of survivors can identify positive factors resulting from the trauma.
LIMITATIONS
-
▪ The number of survivors of the disaster was small.
-
▪ The survivors were all male and self-selected for work offshore.
-
▪ The assessment of lifetime and current PTSD at the same time might have introduced retrospective bias in symptom reporting.
Acknowledgements
Special thanks to Professor J. C. Reid, University of Dundee, Dr P. Rice, Higher Training Coordinator, Tayside Training Scheme, and to both the University of Dundee Postgraduate Department and Tayside Primary Healthcare NHS Trust, for providing the opportunity of a research placement and secondment for A.M.H. to the Department of Mental Health and Centre for Trauma Research, University of Aberdeen. We thank all those who went out of their way to contact other survivors, asking for permission to pass on addresses. Finally, it must be remembered that this study centres on a trauma that cost 167 men their lives and many families their fathers, brothers, sons and loved ones.




eLetters
No eLetters have been published for this article.